
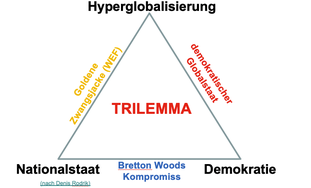
Do you know Schwab’s “Große Umbruch” and Dani Rodrik’s “Trilemma”?
The term trilemma is misused by Klaus Schwab to dismantle human rights, democracy and the rule of law. His “Great Reset” with shock therapy, hyperglobalization and data theft would presumably be disrupted by regional state autonomies and democracy. The fear of Covid-19 should make us docile for the “reset” A real reform is not based on lies. It is much better and nicer: From 2:11:00 onwards at the Corona Committee, episode 28.
Source…

November 18, 2020, by Wolfgang Wodarg
From the beginning of October to mid-November 2020, i.e. within just 6 weeks, the proportion of alleged Covid 19 patients in German intensive care units increased by 15 times. Over half of the beds were suddenly occupied by “Covid-19” patients. The occupancy rate remained almost unchanged. But where are all the other sick people? And why did the RKI find the SARS coronavirus-2 in only 4 percent of outpatients with respiratory diseases (1)? Are there other reasons for the reports of a “Second Wave”? In Germany the performance obviously follows the money.


Pictures from Bergamo
The images from clinics in Wuhan, Bergamo, Madrid and New York created fear that was stronger than all reason. It was they who created acceptance for tough measures. Fear of Bergamo made the government’s intervention in their freedoms seem sensible to many.
In discussions with doctors from northern Italy and with witnesses to the events of March 2020, the Corona Committee shed light on the background to the horror images from Lombardy (2). When in Bergamo, frail and chronically ill people were brought to intensive care units for fear of Covid-19 due to the worsening shortage of nurses, or they – if they did not die there – were put under quarantine in homes with poor care, it was not only the few intensive care units that were cramped and chaotic scenes, but also to a traffic jam at the funeral homeowners. Most of them are said to have been quarantined themselves because of the many contacts. They were also not allowed to bury the dead – as is customary in Italy – but had to have them cremated in the crematorium first.
Many of the elderly people who were abused in this way were only labeled as Covid-19 victims after death using PCR tests, which are said to have had a very high false positive rate. More pictures of ventilated people from the intensive care units, which were chronically overloaded, especially during the flu season, did theirs (3). Such actions produced dramatic images that shocked Europe. They were more convincing to most people than any epidemiological or medical report.
And in Germany? Empty hospital beds create a new emergency
Bergamo was the signal for Berlin. Because at the same time as the lockdown in mid-March 2020, the fear of a supply emergency was fueled, and mood was raised by a priority debate that was drawn by the hair. At the same time, many hospital beds were blocked in order to cope with an announced wave of epidemic victims. A shortage of beds was the alarm call of some triage prophets. Including one who, as a politician in a government group, spread the Bertelsmann message in the summer of 2019: Germany has too many hospital beds (4).
Only half a year later he suddenly stoked the fear of overloading the hospitals with Covid-19 and promised the clinic groups a lot of money as compensation for beds that were kept free. Then came a summer break, during which the viruses were also given a breather and during which our clinics were allowed to collect 560 euros for each empty bed until September (5). Since mid-March, however, many cancer and heart patients have been in need, for example, because access to inpatient treatment was difficult due to the locked beds and some hospitals had sent parts of their staff home on short-time work.
At the beginning of April, the Federal Statistical Office registered a slight excess mortality. Because they were waiting for Covid 19 patients, other patients were not given any appointments and many died because they were not treated or treated in time. Although, as in other countries, the slight excess mortality did not begin until after the lockdown began, the lockdown victims were mistakenly assigned to the “pandemic”.

From March to September, despite an alleged epidemic emergency of national importance, a large part of the beds in the intensive care units of the vast majority of German clinics were empty. They cashed in for empty beds and negotiated with the payers for further advantages in the crisis.
Some clinics did not receive enough compensation for vacancy and others were satisfied and remained silent. In order to do justice to the distribution dispute in the industry, the government, health insurance companies and the hospital industry then backed down slightly without causing a stir and staggered the remuneration for empty beds according to clinic type and region, which led to a slight normalization of patient flows. Here, too, it was shown that clinics are nowadays commercial enterprises and as such react sensibly – but only as such!
How do you make a second wave?
After the many false positive PCR tests had not been reflected in the morbidity statistics of the younger average travelers after the summer vacation, Bergamo seemed to be remembered again and the political motivation boost achieved there. What options do politicians have under pressure to justify themselves to keep a frightened population in line, as in Bergamo, in Bremen, Bielefeld or Berchtesgaden?
In northern Italy you could see, it depends on the images in the media. Whether in Mexico in 2009 or in Wuhan at the beginning of 2020, it was always the images that conveyed the feeling of a “pandemic”. They are apparently more effective than tables, laboratory values, confusing medical records or careful epidemiology. Despite months of research, research, discussions with scientists and despite decades of experience with the pitfalls of infection epidemiology, after all the arduous explanations, I am still told today: “But didn’t you see what was going on in Bergamo?”
Where do the frightening images and narratives come from
Are we being fooled by the current reporting? So far, despite frequent questions, I have not yet found any medical professionals who have ever seen a “second wave” in seasonal respiratory diseases.
It is possible for the media at any time to depict distress, hectic pace and misery in German clinics. The typical scenes in intensive care units have proven their worth. A wired body, lots of hoses, masked and veiled staff and an interview with an exhausted senior doctor, who uses the opportunity to finally get someone interested in the hectic pace, the shortage of staff, the strenuous shift work and the resulting misery for patients and staff . As a hospital hygienist and in the past even a staff representative and intensive care physician, I still have a lot of understanding for such images.
By the way, you die in all intensive care units, always and unfortunately relatively often. If the station is then filled with people over the age of eighty, it was almost a miracle if half of it could be relocated alive.
So if you move many old people to intensive care units and also ventilate invasively, you get Bergamo. Not to mention the risky drug attempts “only for emergency use”.
Does anyone even remember the ideals of palliative medicine? Or was this just a temporary disease industry marketing campaign?
How do you get the elderly into the clinics?
First, ensure that more positive PCR results give the signal that the epidemic is spreading dangerously again. With around 1.5 million tests per week now, nobody can really guarantee the quality of the laboratory anyway. If the polymerase chain reaction (PCR) amplifies something until every test is positive, or if only the E gene is used in the event of a positive reaction, then this can only be seen through by more sensitive team doctors of professional footballers or by stubborn public officials will. No wonder that even before the corona season, which actually only started after the beginning of the year, the positive rate of SARS-CoV-2 PCR mass tests could be increased from a little over 1 percent to almost 8 percent within 6 weeks.
There are obviously big differences between the laboratories, but the RKI did not want to provide any information when asked. From the very beginning, the PCR test had little to do with diseases. The secret motto still seems to be: More tests = more false positives. And the more negligent a laboratory, the more happy those responsible are about a high hit rate to confirm their scare tactics.
Concerted action care and Covid-19
If you do notice, you can combine the practical with the useful and change the test strategy again. That too has happened gradually over the past few weeks. With fewer tests, more hits and more fear of the disease? That’s fine. For example, when I test staff in retirement homes or clinics, it has an enormous effect.
Every “case” with the staff leads to a temporary work ban, to an investigation of possible contact persons and thus automatically to a deterioration of the staff code. The already overloaded staff suffers from this and already has to work up to 60 hours a week. And of course the residents and those in need suffer even more. This is twice as bad if relatives or friends are also not allowed to visit. Everyone is constantly talking about protecting particularly vulnerable groups. However, the regulations put in place put the elderly and needy people affected in a precarious position and isolate them to a large extent in their mostly painful loneliness in the home.
My colleague at Transparency, Adelheid von Stösser, is also a courageous fighter for the rights and quality of life of old people and people in need of care. In her Zeitschrift für Pflegeethik (6), she described the very moving fate of these victims when they were locked down for the first time and is appalled by the brutality with which hygiene plans put the vital needs of people in their retirement years and thus deprive many of those affected of their courage to face life.
It therefore seems macabre when three ministers praise their “Concerted Care Action” at a press conference during the corona crisis and at the same time increase the distress of the dependent residents and the stress of the remaining caregivers to unbearable levels by means of lockdown, targeted test and quarantine measures for nursing staff and visiting bans .
Beware, they presume to protect you!
So if you now prescribe mandatory tests for employees “to protect vulnerable groups” in residential complexes for the elderly and homes, you will certainly tear a deep gap in the care structures. With a positive rate currently averaging (!) Almost 8 percent, considerable gaps in care and a deterioration in care are to be expected. Was the calculation when you defined a focus for the future test strategy?
Because of the “nursing emergency”, the health minister had advocated strengthening these important professions in nursing. And now that? Whether a test is true or false positive certainly does not play a role for the nursing staff, because healthy people who are fit for work are tested at work. You only need to find 8 percent “positives” to open up a huge quarantine gap among the employees and those in care.
From Bergamo to Bavaria – that’s how it works
If a large part of the nursing staff then has to stay healthy but “positive” at home, we come a little closer to Bergamo. Old people and those in need are undersupplied because of a lack of staff, sedated, dry out – risk of thrombosis and embolism! – or are immediately admitted to the clinic “to be on the safe side” or because of a positive test result. So if the elderly and chronically multimorbid people are shoveled into the clinics by means of a test, one can imagine which images can be staged for the fear mongers. Here is an alarm call from Bavaria on November 11, 2020 (7):
“Since patients / residents and staff have been systematically tested, it has happened that from now on half of the staff is eliminated because they either tested positive or were contact persons. As in the hospital in Schongau, where 600 employees were quarantined for at least 10 days at the end of October and the clinic was temporarily closed. One can only imagine what this means for the patients who are lying there and cannot be moved to other houses so quickly. “
The tests – a win-win business at the expense of third parties
If you want to fuel these emergency and panic situations in order to scare us, you only have to ensure that more testing is carried out on an outpatient basis and in care facilities. In institutions, this is simply ordered by the legislator, then the positive domino will soon run nationwide by itself. But there is also a tried and tested means of increasing cooperation between the medical profession in statutory medical practices: More money! It is now being printed en masse and no longer seems to play a role. A resident statutory health insurance doctor reported to me indignantly how this would affect me. He writes:
“At first there was not a cent for the tests and many colleagues (almost all of them in the region) hardly tested at all. Now we get more money (15 euros) for a test (duration 1 min) in healthy people than for a complete abdominal sonography for an acute abdomen (15 min for 12 euros). That’s why all of a sudden testing is taking place everywhere. “
Our health care system is managed “with the golden reins”, as the impartial chairman of the Federal Joint Committee (GBA) Professor Joseph Hecken once explained to me. This means that money is used to set the incentives for what patients then have to experience or have to pay for.
Hospital profit center
Financial disincentives seem to be even more devastating in hospitals. In the large clinic groups in particular, the flat-rate case fees that have been politically pushed for years by pseudo-leftist health economists have made money the most important driving force behind the clinic. Institutionalized – that is, legalized – corruption flourishes there. With bonus payments for chief physicians, with the monopoly of supply chains or through skillful collaboration with pharmacies, medical device manufacturers and pharmaceutical companies, more and more expensive services are provided and billed. Not because patients absolutely need them, but because they can optimize the financial results of the hospital clinical profit center.
“If we don’t generate a double-digit return, we’ll close the shop here,” the managers of the Helios chain had bluntly given me during a visit with Karl Lauterbach in their clinic in Damp on the Baltic Sea. My real concern at the time was that this clinic should open up more to the inadequate emergency care in the country, but I was probably too naive then, as the member of the Rhön Clinics’ supervisory board, Comrade Karl Lauterbach, made me understand with a reproachful smile .
But not only in the governing parties did and still have a deeply rooted lobby. Now in the Corona crisis it has paid off. In my opinion, such lockdown nonsense can only be actively and actively participated in by someone who expects something from power or money or both, or who is afraid of losing this if he refuses. At the corporations in the health industry, everything is running smoothly, or as if it were lubricated, with golden reins.
Wages of the fear makers
Most clinics are already doing the Corona hype anyway because their lobby has ensured that a large part of the tax money and contributions thrown out the window for Covid-19 ends up at the clinics since March.
Initially, in March 2020, they achieved that a corona surcharge of 50 euros per day was paid for each occupied bed. The already mentioned empty bed fee of 560 euros per day was also brilliant. For every newly installed intensive care bed, there was even a grant of 50,000 euros. Even when they weren’t needed, many homes took this business away. Empty beds need few staff and still bring good money in times of Corona. After the first lockdown turbulence, Covid-19 was not noticeable in the stationary sector. The occupancy of intensive care units in Germany from March to the end of September 2020 averaged 50 to 75 percent. That has hardly changed so far. But the diagnoses reported there.
The new strategy
One switched. On October 12, the clinics received further financial incentives retrospectively from October 1, 2020, so that the occupancy of the free beds is more profitable again, but only for Covid-19 cases that tested positive. According to Section 5 (3i) KHEntgG for 2020 (Corona additional cost surcharge agreement 2020), the legislature granted them significantly higher surcharges. At the same time, the medical service should turn a blind eye in an “emergency” and only check less than half as often what is being done with our money. For every treatment case with a positive test result and for every case with clinical symptoms that can be interpreted as Covid-19, there is an additional 100 euros Covid-19 per day from October 1, 2020 until the end of the “epidemic emergency of national scope” -Special fee.
This attractive offer came, in parallel with the test orgy in care facilities and in view of the expected assignments of suspected Covid 19 cases, just in time and has apparently been used by the clinics to a surprisingly large extent since October 1st. Even if the utilization of the intensive care units – if only because of the shortage of staff – did not change significantly overall, the proportion of “Covid-19 cases” rose rapidly to an average of around 50 percent. From the beginning of October to the middle of November, i.e. within just 6 weeks, that was an increase of 15 times! The proportion of ventilated Covid-19 cases of 56 percent is alarming. Hopefully many of the 2010 invasive ventilators are only because of a positive test result, So with and not primarily because of Covid-19 in these statistics. Invasive ventilation of patients treated as Covid-19 has now proven to be a life-threatening additional risk worldwide.
I would like to know from the health insurances how the age distribution of intensive care patients has changed since mid-September and what happens to the proportion of patients from old people’s facilities. I’m still waiting for this data. The cost bearers must have stumbled upon this development long ago, but the bodies responsible for monitoring misconduct in the health insurance funds seem to prefer not to look very closely at this “Great Reset” of bed occupancy.
The above shows once again that hospitals have primarily mutated into commercial enterprises in which economic thinking determines the decisions. As a welfare state, however, we are a constitutional community based on solidarity. We carry our contributions in solidarity to the best of our ability in order to be able to help those who need help. That is also the principle of our health system. It is based on the principle of solidarity and was also a public task in the area of administration and ensuring adequate supply. When cities, districts and federal states leave the general care for health to large monopolists and thus get rid of their responsibility for the sick and the elderly, then it will soon no longer be about health, but only about money,
The “Great Reset” in healthcare seems to have been over long ago. The “economic hitmen” have been with us for a long time and what we are experiencing now is only a symptom of the progressive deregulation of our common good over the past few decades. When the common good abolishes itself, well-organized egoists take over the regime with a fatherly gesture, and democracy has a hard time.
But I have a dream!
Sources and Notes:
(1) The RKI reports on November 17, 2020:
In the outpatient area, the activity of acute respiratory diseases (ARE rates) in the population in the 45th week of 2020 has slightly decreased nationwide compared to the previous week.
Two (4 percent) of the 51 sentinel samples examined were positive for SARS-CoV-2.
But in the inpatient area, the total number of treated cases with acute respiratory infections (SARI cases) has increased further. The proportion of COVID-19 diseases in SARI cases has risen sharply and was 49 percent in week 44, 2020.
(2) https://youtu.be/Qmls6bj2jxI
(3) https://www.wodarg.com/covid-19-in-italien/
(4) https://www.augsburger-allgemeine.de/politik/SPD-Gesundheitsexperte-Lauterbach-Wir-haben-zu-viele-Krankenhaeuser-id54513861.html
(5) Covid-19 Hospital Relief Act of March 27, 2020:
Hospitals receive financial compensation for postponed scheduled operations and treatments in order to keep capacity free for treating patients with coranavirus infection. For every bed that is not occupied between March 16 and September 30, 2020, the hospitals receive a flat rate of 560 euros per day. The compensation is paid from the liquidity reserve of the health fund, which is refinanced from the federal budget. They also receive a bonus of 50,000 euros for every additional intensive care bed they create. The costs for this are financed from the liquidity reserve of the health fund. In addition, the federal states are to finance further necessary investment costs in the short term. For additional costs, Particularly for personal protective equipment, hospitals will receive a surcharge of 50 euros per patient from April 1 to June 30, 2020, which can be extended and increased if necessary. The so-called “provisional maintenance fee” is increased to 185 euros.
(6) http://pflegeethik-initiative.de/2020/04/15/corona-krise-falsche-prioritaeten-etzt-und-ethische-prinzipien-verletzt/
(7) https://www.merkur.de/lokales/schongau/schongau-ort29421/schongau-krankenhaus-corona-ausbruch-mitarbeiter-angefeindet-90092945.html
more…