
By Torsten Engelbrecht, co-authored by Claus Köhnlein, MD
When the Australian state of Victoria with its capital Melbourne recently showed the world what a lockdown of the hardest kind looks like—with orders such as the police being allowed to enter anyone’s home without a warrant, an 8 o’clock curfew, or even a ban on weddings—Jeffrey A. Tucker, editorial director of the American Institute of Economic Research, commented: „Melbourne has become a living hell. Tacitus’s line about the Roman empire comes to mind: ‚Where they make a desert, they call it peace.‘“
Source…
Indeed, such constraints are all the more a farce because lockdown measures of any kind do not have a scientific foundation and already contradict the common sense. The rigid stare on an alleged potentially deadly virus named SARS-CoV-2 prevents that the true causes, especially of the so-called COVID-19 deaths, come to light: The experimental administration of highly toxic drugs.
The mere fact that „in Australia since March, there have been 50 percent more deaths from suicide than official numbers show for Covid-19,“ as Tucker points out, should give everyone plenty to think about. Or let’s take outdor air pollution: Though it causes more than 3 million premature deaths a year worldwide, the decision makers do not come up with the idea of paralyzing the fine dust polluters via lockdown.
Apart from that, so-called SARS-CoV-2 tests, whose „positive“ results are being used as the rationale for the lockdowns, are in fact scientifically meaningless. This is illustrated already by the fact that there is not even a valid gold standard for these tests, as for example Australian infectious diseases specialist Sanjaya Senanayake confirmed in an ABC TV interview.
Yet, Australian government’s own website admits COVID-19 PCR tests are totally unreliable. And then studies also show that lockdowns and mask mandates do not lead to reduced COVID transmission rates or deaths.
A lockdown in Australia is all the more absurd if you consider that there „the per capita deaths are about 26 per million over a six months period,“ as David James, journalist from Down Under, stated recently in an OffGuardian article. With the best will in the world this cannot be called a virus pandemic. Especially since „The chief health officer in Victoria admitted that they were not testing for the virus, just assuming that if there were flu-like symptom it must be COVID-19; and deaths by flu in Australia, it should be added, are running unusually low,“ as James adds.
Moreover, many countries did not record any excess mortality in the first six months of 2020, while in Germany or Portugal, for example, the mortality rates for this period are even below that of the one or the other previous year. This is the result of an analysis titled „For [the decision makers] know not what they do“ done by Stefan Aust, former editor-in-chief of Germany’s best knownnews magazine Der Spiegel and since 2014 publisher of the German daily newspaper Die Welt.
That Germany and other countries do not experienced an excess mortality, this could not be considered a success of the governments‘ lockdown measures, as Aust expounds. A main reason: For the majority of those who were declared as corona deaths was very old and came from the care sector of the most seriously ill. And „their lives could not have been saved even with the strictest general social lockdown measures.“
Excess mortality rate was limited to a very short period of time, which make nonsense of the virus hypothesis
Sure, some countries recorded noticeably more deaths in the first half of 2020 than in previous years. This holds especially for Italy, Spain, France, England, Belgium, the Netherlands and the USA. However, the hypothesis that a new, potentially deadly corona virus would have raged in these countries is already contradicted by the fact that these states in particular pursued a rigid lockdown policy. Therefore, following the logic of the virus, they should have had fewer deaths.
In addition, Belgium, for example, had eight times more deaths (per 100,000 inhabitants) than its neighbour Germany, Spain 22 times more than Poland, while Portugal, Spain’s direct neighbour, did not experience any excess mortality. But a virus pandemic, which afflicts countries so differently, cannot actually exist, especially in today’s times.
This is why my co-author, Claus Köhnlein, MD, stated in a letter, published at the end of June in the German Ärzteblatt (medical journal): „In view of the fact that very different mortality rates are reported in different European countries, it is reasonable to assume that a differently aggressive therapy could be responsible for this.“
This is also clearly supported by the fact that the very largest part of the excess mortality in these countries only took place during a very short period of time, within about two to three weeks around early/mid-April. As the Euromomo death rate statistics show, also in these countries the graphics had been relatively „boring“ until around end of March, but then the excess mortality suddenly shot up, only to drop drastically again around mid-April—whereby the majority of the humans concerned were of old age (see the charts below in which the „prongs“ in the charts of Belgium, France, Italy, Spain and UK are clearly visible).
Z-score for various European countries, Dec. 2019 – Sept. 2020


Source: www.slideshare.net/lschmidt1170/europe-map-study

Source: https://www.euromomo.eu/graphs-and-maps/#z-scores-by-country
As the graphs clearly show, in the first half of 2020 excess mortality occurred only in a few European countries, mainly in Italy, Spain, Switherland, France, Belgium and England (recognizable by the “prongs” in the curves). These graphs provide the irrefutable evidence that this phenomenon cannot be linked to a new potentially deadly virus. For not only did the excess mortality occur only within a very short period of time, with a steep rise and equally steep fall in the mortality curve within two to three weeks in April – and thus also outside the usual flu season. No virus can produce such „prongs“. Also, in Germany, for example, though it borders directly on France and Belgium, no excess mortality occurred. The same applies to Austria, which directly borders to Italy and Switzerland, and Portugal, which is the neighbor of Spain. And while Italy, Spain, France, Belgium and England had a short, noticeable excess mortality rate, THOUGH they had implemented a hard lockdown, Sweden, which did not introduce a lockdown at all, only had a very slight excess mortality rate. Even this cannot be explained with the best will in the world with enem virus. By the way, the reason why the „prong“ in Switzerland is relatively flat is that the German speaking part of the alpine country, where there was practically not excess mortality, two thirds of the total population live, whileexces mortality was recorded in the Italian and French speaking part. So has the virus simply avoided the German-speaking Swiss? A completely abstruse idea!
In numbers this means that within a few weeks 60 to 70 thousand more deaths occured in these European countries than usual at this time of the year. Plus around 130,000 additional deaths in the US during the first six months of 2020 compared to the same period of the previous two years (the death rate in the USA for the first half of 2020 is 0.48 percent, in 2018 and 2019 it was 0.44 percent ). The only difference between the European countries and the United States ist that the „prong“ in America is a bit wider, i.e. it does not only extend over about two April weeks, and that its peak of excess mortality is on April 11, about two weeks later than that of Italy, where the worldwide death drama started (see chart below).
Weekly number of actual deaths in the United States from all causes
compared to the maximum expected number (June 2018 – Aug. 2020)
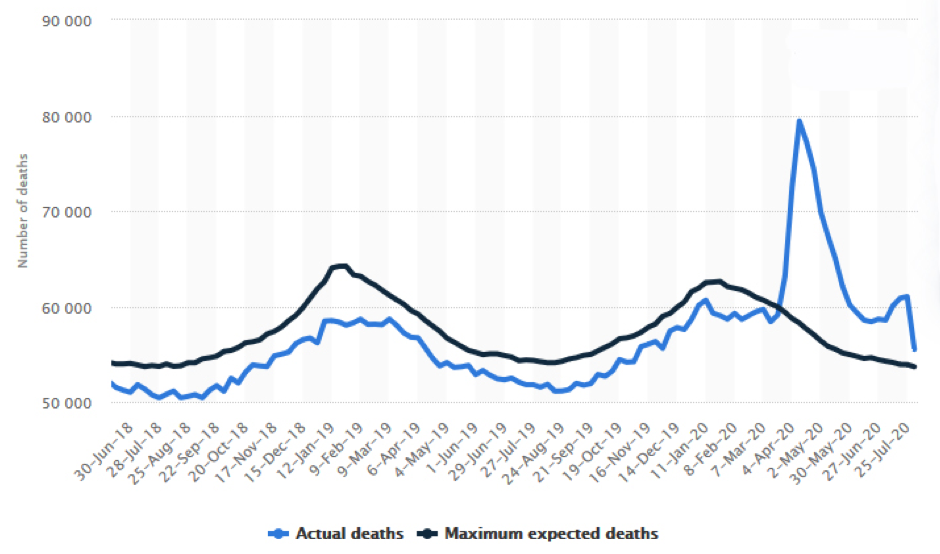
This finally makes it impossible to explain that it was a virus that killed many tens of thousands in exactly two weeks out of season. Such a virus simply cannot exist. And even such a super deadly virus existed, then it would have to cause a staggering „prong“ in the chart of Sweden, a country that did not lock down at all. But you can only see a flat hump in mid April in the Swedish chart.And the death rate, i.e. the share of deaths in the total number of inhabitants, in Sweden for the first six months of 2020 is with 0.48% absolutely in the range and only slightly higher than in 2017 and 2018 (0.46%), for example.
This is why there can only be a non-viral explanation for this temporary massive excess mortality. And there is solid evidence that the massive and high-dose administration of highly toxic drugs plays the decisive role—drugs that have been used in worldwide trials and also beyond these trials, costing the lives of tens of thousands of test persons. In the course of time the „patient supply“dried up which explains the rapid drop in the curves creating these „prongs.“
A closer look at Germany reveals this as well. The Euromomo chart above for Germany is actually limited to the capital Berlin. But the data from the German Federal Office of Statistics shows the weekly death rates in detail (see chart below). And this chart tells usthat in March 2019, for example, about 86,500 people died. „In March 2018, i.e. in a year when the flu epidemic was particularly severe, the figure was 107,100. Even without a corona pandemic, the death toll can therefore fluctuate considerably, especially during the typical flu season,“ as it says on the website of the Federal Office of Statistics. Hence, a coronavirus death train cannot be derived from the 2020 curve with the best will in the world.
Weekly death rates in Germany (2020, 2019, 2018, 2016-2019)

The graph discloses as well that also in Germany there was a „prong,“ but it is seen only in the same short period of time (in April) as in the other countries, which, as mendioned, reduces the virus hypothesis to absurdity. Moreover, the „prong“ is relatively flat. In April 2020 there were almost 6,600 more deaths compared to April 2019 and almost 4,200 more than in April 2018. And „since the 19th calendar week (May 4 to 10) [of 2020], according to the preliminary count, the death figures were initially back in the range of the average of previous years or fluctuated around it“, as it also says on the website of the German Federal Office of Statistics. „By mid-July, the death figures had reached a minimum. In August, however, the mortality figures had increased again in the course of the heat wave.“
The flat „prong“ in the 2020 chart of Germany with an excess mortality of a few 1,000 in April (compared to 2019 and 2018) corresponds almost exactly with the increased experimental use of the malaria drug hydroxychloroquine in so-called COVID-19 patients (more on the crucial role of this drug later). As the German news magazine Spiegel reported some days ago, according to an analysis of the German health insurance AOK the drug had found many supporters also in Germany from March on. In this month the drug was prescribed to almost 10,000 more patients than in the previous month—patients, the vast majority of whom were very old and had serious health problems and for whom highly toxic drugs were therefore particularly life-threatening. In April and May, the numbers for hydroxychloroquin administration in Germany dropped again. In June, the figures were then below the average of the previous year.“
In fact, it seems not very likely that in Germany in connection with the general COVID 19 panic, which was particularly glaring in the second half of March, there was no increased experimental use of various highly toxic medication. And it is also remarkable in this context that on March 24, shortly after an interview with my co-author Claus Köhnlein, MD, was broadcasted on YouTube on March 20, in which he criticized the experimental use of highly toxic drugs (the interview had 900,000 views within a short time), he received a phone call from a then Charité doctor named Felicia Kleimaier.
Kleimaier asked Claus Köhnlein if he was aware that his critical statements had torpedoed the application of the antiviral therapy inconnection with COVID-19. His answer: If his interview statements had really contributed to the fact that significantly less medication was used, then he would have reached exactly what he wanted to achieve, because such a therapy is always immunosuppressive and thus can be fatal, especially for already severely ill people.
In the mentioned letter to the journal Ärzteblatt my co-author also wrote: „It could be that we in Germany got off so well because we were therapeutically more reserved from the beginning and because of the bad experiences of Italy, Spain, France and England and therefore hardly used any immune suppressive antiviral substances.“
Lancet case study from February 18, 2020:
A blueprint for medication excesses
That there was a massive experimental use of medication, this became possible also due to papers such as the single-case study that was published in The Lancet on February 18th. It describes a casuistry of a 50-year-old patient who suffered from fever, chills, coughing, tiredness and shortness of breath and who has been classified as COVID-19 patient.
Thereupon he was treated with a real drug armada consisting of the antiviral drugs interferon alfa-2b, lopinavir and ritonavir, the very hard antibiotic moxifloxacin and high dose of cortisone (methylprednisolone)—substances that can have lethal side effects even when taken alone. Moreover, tissue samples were taken during the autopsy—and here the authors even concede that the observed liver damages may have been caused by the drugs. The conclusion that the patient died due to drug toxicity is inevitable.
And if this man who was „in his best years“ at the age of 50 and who had suffered apparently from no other illnesses than severe flu symptoms, dies after the administration of such „drug cocktail,“ then one can guess how such a highly toxic treatment affects peopleclassified as COVID-19 patients in their 70s or 80s with previous illnesses up to cancer.
But why the attending physicians treated the 50-years-old this way? Out of a virus tunnel vision, the deep-seated belief that only drugs can bring salvation and out of the fear, typical for today’s medical system especially in times of pandemic panic, that one could have left a remedy untried, which then often enough leads to drug actionism. As in this case.
Because the pitful 50-years-old was short of breath, he was given for example cortisone, a lymphocyte killer that slows down the inflammatory response. Everything then detumesces, the fever goes down. The patient feels temporarily better, he can breath better again. At the same time, however, the defence reaction is suppressed, which can finally end up being fatal, as can be seen in this case, especially if other potentially lethal medication is administered in addition.
Nevertheless, the Lancet study concluded: The „patient.. died from severe infection with… SARS-CoV-2.“ In other words: The patient was claimed to have died only of a virus and despite the drugs not because of the drugs. And this kind of study, published in a journal whose content is de facto law, served as blueprint for the treatment of COVID-19 patients.
In fact, only a few weeks later, highly toxic and also potentially lethal drugs were used excessively, especially in all of the above-mentioned countries with excess mortality, both experimentally and off-label, meaning that the drugs were used outside of their regulatory approval—and this in people, most of whom were old and had serious illnesses, before being tested „positive“ for COVID-19.
The avalable data gives the impression that increased deaths migrated like a huge wave within a short time from Italy via Spain and France to the UK and Belgium and then spilled over to the USA and Brazil.
In Italy, especially in Lombardy, the „drug frenzy“ started on March 17th at the latest, and it took place in homes, nursing homes and clinics. For Italy, there is a death statistic dated April 9, 2020, which states that 84% of the deceased patients received antibiotics, especially azithromycin, 55% got antiviral drugs, 33% corticosteroids and 18.6% a combination of all three.
Re azithromycin, the U.S. Food and Drug Administration (FDA) is warning the public that it may lead to a potentially fatal irregular heart rhythm. And the fact that antiviral drugs can be lethal has also been sufficiently proven. This also holds for the combination Lopinavir-Ritonavir, which was also given to the 50-year-old patient mentioned above.
And as for corticosteroids, a study published in the Journal of Infection on 10 April 2020 concluded: “Patients with severe conditions are more likely to require corticosteroids. Corticosteroid use is associated with increased mortality in patients with coronavirus pneumonia.”
France Culture described how this was done in practice in an article titled „Covid-19: in France, Italy, Spain, Germany, how doctors are tackling the disease,“ by quoting the neurologist Francesco Alberti, president of the Order of Physicians of the Province of Imperia (a subdivision of the Liguria region bordering France), who had returned to work due to the pandemic:
“We are doing a lot of experimentation and many trials, because the disease is very different and more or less serious depending on the patient. If there is only fever and it doesn’t last more than 4 or 5 days, we prescribe paracetamol. Beyond that, we use antivirals to limit the progression of the disease: the most commonly used drugs are hydroxychloroquine, brand name Plaquenil, combined with an antibiotic, azithromycin, bearing in mind that hydroxychloroquine can cause heart rhythm problems. We also give other antivirals such as remdesivir and favipiravir. In case of immune system runaway, we are also experimenting with tocilizumab, an immunological drug usually prescribed for rheumatoid problems.“
We will discuss hydroxchloroquine, its deadly potential and its decisive role as well as remdesivir later. As far as tocilizumab is concerned, it can be deadly just like azithromycin, by causing lethal allergic reactions. Since this immunosuppressive drug was launched in the US in 2010, more than 1,000 deaths have been reported to the FDA. However, the actual number is likely to bemuch higher as the FDA’s reporting system only covers a fraction of the adverse events that occur in patients.
Meanwhile Alberti continued: „There is no single therapeutic protocol. The drugs we use are ‚off label‘, i.e. we prescribe them outside their indications. The Ministry of Health and the Italian Drug Agency have authorized us to use these drugs, even if they were originally prescribed for other diseases.“
Jean-François Timsit, Head of the Department of Intensive Care Medicine and Resuscitation of Infectious Diseases at the Bichat Hospital in Paris, for his part said: „For the moment, the mortality rate is estimated at around 30 percent for patients who are in intensive care, with a variation depending on whether or not patients are intubated [for machine ventilation]. When patients are intubated, the death rate rises to 50 percent.“
30 percent is already a very high figure, 50 percent all the more. In fact, intubations (introduction of holoprobes) were increasingly used because it was feared that the significantly less invasive mask respiration would carry a higher risk of viral infection. And this, though the fact that patients died more frequently as a result of this has already been documented in relation to SARS in 2002/2003.There is also clear evidence of this in the treatment of COVID-19 patients. A Lancet study from February drew a very bleak picture: only three out of 22 intubated patients survived.
In terms of drugs, hydroxychloroquine which has already been administered extensively to patients in Italy, has played a significant part in making countless people die prematurely. Hydroxychloroquine is by far not a candy, it can have many serious side effects and even be fatal by causing cardiac arrhythmias, for example. Especially if it is given in higher doses, which is exactly what happened in the treatment of so-called COVID-19 patients, not only in Italy, but also in Spain, France, England and the USA. “I agree about hydroxychloroquine overdosing, both from a reduced function point of view and toxicity,” writes us Yale epidemiologist Harvey Risch, who is one of the best known researchers who see a potential curative effect in the drug if administered in low doses, by e-mail.
In Spain, the Agencia Española de Medicamentos y Productos Sanitarios (AEMPS)—the Agency of Medicines and Healthcare Products—started the extensive distribution of hydroxychloroquine and its somewhat more toxic variant chloroquine for COVID-19 in hospitals on March 16, through the application of Management of Medicines in Special Situations (MSE). As Miquel Barceló from the hospital Cerdanya around 150 km north of Barcelona and directly at the border to France told France Culture at the beginning of April: “There is a more or less reckless behavior in relation to this drug [hydroxychloroquine]… There are many patients in intensive care and many deaths compared to Occitania [directly on the opposite French site]… Faced with this drift of the disease, people say to themselves: we must do something. There is perhaps less stopping to use this drug.”
March 18, 2020: WHO Director General Ghebreyesus sounds the experimental drug attack
On March 18, Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, had proclaimed a major study-based and medicamentous offensive to fight COVID-19:
“Multiple small trials with different methodologies may not give us the clear, strong evidence we need about which treatments help to save lives. WHO and its partners are therefore organizing a study in many countries in which some of these untested treatments are compared with each other. This large, international study is designed to generate the robust data we need, to show which treatments are the most effective. We have called this study the SOLIDARITY trial.”
And the focus of this Solidarity trial was on the following already mentioned highly toxic drugs: remdesivir, lopinavir/ritonavir (Kaletra), Interferon-β in combination with Kaletra and hydroxychloroquine and chloroquine.
“However, the doses were not specified on WHO’s list of the drugs to be trialed, nor were the actual doses specified, surprisingly, in WHO’s consultation on chloroquine dosing, dated April 8,” as Meryl Nass, a physician from Maine, points out in an article for the Alliance for Human Research Protection.
Instead, the introduction of the report of that meeting notes, “The chloroquine or hydroxychloroquine schedule selected for the trial includes two oral loading doses (250 mg per tablet CQ or 200 mg per tablet HCQ), then oral twice-daily maintenance doses for ten days. This meeting convened to discuss the appropriateness of the selected doses for the trial.”
But according to Nass, this statement about “dosing seems to be deliberately vague or even misleading, as the actual dose used in the Solidarity trial is 2,400 mg during the first 24 hours, and a cumulative dose of 9.2 grams over 10 days.”
This extremely high dose is all the more strange when you consider that a document of the WHO’s March 13 informal consultation on the potential role of chloroquine shows that the Gates Foundation had been studying chloroquine’s pharmacokinetics (of the 25 participants at this meeting, 5 were from the Gates Foundation). And in this file it says “Higher doses would be considered for treatment, i.e., 10mg/kg base, followed by 5mg/kg twice daily for seven days.” That is to say, a typical 70 kg person would, if this suggestion had been followed, receive 700 mg base, which equals 900 mg of chloroquine, as a loading dose, being light years away from the dose used in the Solidarity trial of 2.4 g in the first 24 hours.
Note that both, chloroquine and hydroxychloroquine, are very difficult to break down, so the doses have a cumulative effect, and they are used in euthanasia. In 1986, the German journal Zeitschrift für Rechtsmedizin published the article „Tod nach Gabe von 1250 mg Chloroquin bei Porphyria cutanea tarda“ (Death after administration of 1.25 g chloroquine in [the metabolic disease] Porphyria cutanea tarda). Other sources put the lethal dose at 2 to 3 g.
In 1979, the WHO hired a consultant named H. Weniger to explore the toxicity of ychloroquine. He looked at 335 episodes of adult poisoning by chloroquine. Weniger on page 5 notes that a single dose of 1.5 to 2.0 g of chloroquine base [= equivalent of 1.9 to 2.6 g chloroquine] may be fatal.” And the dose used in the Solidarity trial was, this should be mentioned here again, 2.4 g in the first 24 hours alone.
According to Nass, “All experts agree that ‘chloroquine has a small toxic to therapeutic margin,’” as it can be read in Goldfrank’s Toxicologic Emergencies. “It is very safe when used correctly in the right patients,” writes Nass, “but a bit more can potentially kill. Professor Nicholas White, who attended both WHO consultations on the chloroquines, has mentioned this.”
This is aggravated by the fact that the WHO report of its meeting on chloroquine dosing states, “Although the preponderance of opinion tilted towards a reasonable benefit risk profile for the intervention, there was some scepticism about what was considered a ‘minimalistic safety data collection’ currently included in the protocol.” Nass’ commentary: “The high dose regimen being used in the Solidarity trials has no medical justification. The trial design, with its limited collection of safety data, may make it more difficult to identify toxic drug effects, compared to standard drug trials. This is entirely unethical.”
Nevertheless, many countries around the globe joined the Solidarity trial, among them Spain, France, Switzerland and Belgium—countries with a noticeable excess mortality (limited to April).
At the end of March, also none other than US President Trump praised hydrochychloroquine as “a gift from God,” which certainly has given the desire for this drug and the belief in their possible healing power an extra boost. But as promising the well-meaning name “Solidarity” and Trump’s glorification sounded, the whole thing ended in disaster, also due to the overtherapy with hydroxychloroquine, which in many cases has been given together with other toxic drugs.
How fatal chloroquine was, was demonstrated in Brazil. On April 13, the Chicago Tribune reported that a study in Brazil where “national guidelines recommend the use of chloroquine in coronavirus patients” was halted early for safety reasons after coronavirus patients taking a higher dose of chloroquine developed irregular heart rates that increased their risk of a potentially fatal heart arrhythmia. Patients in the trial were also given the antibiotic azithromycin, which carries the same heart risk.
“To me, this study conveys one useful piece of information, which is that chloroquine causes a dose-dependent increase in an abnormality in the electrocardiogram that could predispose people to sudden cardiac death,” said Dr. David Juurlink, an internist and the head of the division of clinical pharmacology at the University of Toronto, referring to an electrocardiogram, which reads the heart’s electrical activity.
Roughly half the study participants were given a dose of 450 milligrams of chloroquine twice daily for five days, together 4.5 g,while the rest should get a higher dose of 600 milligrams every 12 hours for 10 days, together 12 g. Within three days, researchers started noticing heart arrhythmias in patients taking the higher dose. By the sixth day of treatment, 11 and thus a considerable part of the test persons had died, leading to an immediate end to the high-dose segment of the trial.
Switzerland: Only German-speaking part spared from excess mortality
The fact that practically only drugs provably come into question as major cause for the observed excess mortalities was particularly evident in Switzerland. In this country 16 hospitals joined the Solidarity study, among the University Hospital of Lausanne. The reason is that in the alpine country deaths came mainly from the Italian-speaking Ticino and the French-speaking part of the country, while the German-speaking region was largely spared, as data from the Federal Statistical Office show. And the German speaking canton of Zurich with its 1,521,000 inhabitants had fewer deaths than Ticino having a fraction of the Zurich population (353’000 inhabitants). The idea that a virus could attack ethnic groups in such different ways, is just completely irrational.
The deaths also occurred almost “blazing fast”, which also clearly speaks against the virus hypothesis. This is what happened for example in the St. Antonius retirement and nursing home in Saas-Grund. As Swiss television reported, the first „positive“ test came on April 1, the first death on April 17, and shortly afterwards another 14 died, i.e. a total of almost a third of the home’s residentspassed away very rapidly. “We had many inhabitants, who were relatively well on the way with the virus, and we had actually seven to eight days the feeling that the people were over the hump, and suddenly things went very badly,“ so the housemaster Patricia Pfammatter. „Within a few hours they were then partly no longer responsive, terminal, you could tell they were coming to an end.“
„It appears that the Solidarity trials are not testing the benefits of hydroxychloroquine on Covid-19, but rather testing whether patients tolerate toxic, nontherapeutic doses,“ as Meryl Nass criticizes.
France: A lot of drug experimentation
Notabene, the Solidarity studies weren’t by far the only experimental trials. On Marach 22, INSERM, the French biomedical research agency, announced it will coordinate an add-on trial in Europe, named Discovery, that will follow WHO’s example and will include 3200 patients from at least seven countries, including 800 from France. It was said, the trial would test the same drugs, with the exception of chloroquine.
On April 8, Newsweek reported that the University Hospital in Nice (CHU), which had been selected for the Discovery study on March 22, had to stop an experimental treatment with hydroxychloroquine. In an interview with the French daily newspaper Nice-Matin, Emile Ferrari, Head of Cardiology at the Pasteur Hospital, which is part of the CHU, stated that some patients should have discontinued treatment because of the risk of cardiac arrhythmia. According to Ferrari, the cardiac risk is increased if the antibiotic azithromycin is given in addition. For some patients, who are treated with these medicines, the medicine is more harmful than the illness itself, stated Ferrari. “The new observations are quite significant, as the combination is currently being tested in numerous other COVID-19 studies,” as the German journal Deutsche Apotheker Zeitung (German Pharmacists Newspaper) reported.
As far as France is concerned, massiv drug experimentation had taken place there as well. On March 23 the newspaper L’Express reported that the High Council of Public Health (Haut Conseil de santé publique) “encourages doctors to include as many patients as possible in the various therapeutic trials underway in our country because it is the surest way to quickly determine whether a treatment is effective or not.” And according to a list of different kinds of COVID-19 therapy projects first published on April 1 various drugs, among them remdesivir, Kaletra or hydroxychloroquine, are mentioned.
And as an official Belgian guideline document issued June 8, 2020, shows, high doses hydroxychloroquine were used also by the Discovery trial in the EU and by the WHO.
Hydroxychloroquine dosage in Recovery trial on a lethal level
We are far from reaching the end of the study road! On April 3, the UK government announced, „almost 1,000 patients from 132 different hospitals [in the UK] have been already recruited in just 15 days and thousands more are expected to join the Randomised Evaluation of COVID-19 Therapy (RECOVERY) trial in the coming weeks, making it the largest randomised controlled trial of potential COVID-19 treatments in the world. The trial is testing a number of medicines. They include: Lopinavir-Ritonavir, [the anti-inflammatory drug] Dexamethasone, Hydroxychloroquine.“ The Recovery trial was also designed to test the already mentioned azithromycin and tocilizumab as well as REGN-COV2, described as „a combination of monoclonal antibodies directed against coronavirus.“
The Recovery trial—funded in part by the Welcome Trust and the Bill & Melinda Gates foundation—has proceeded at unprecedented speed, enrolling over 11,000 patients from 175 NHS hospitalsin the UK within a relatively short period of time. But then, the hydroxychloroquine arm of the study was discontinued. The rationale was: „These data convincingly rule out any meaningful mortality benefit of hydroxychloroquine in patients hospitalised with COVID-19.“ But this was an euphemism that completely distorted reality, because not less than one quarter (25.7 %) of the people treated with hydroxychloroquine have died.
In fact, this is not really surprising when you look at the hydroxychloroquine dosage which resembles the one of the Solidarity trial. As Martin Landray, professor of medicine at the University of Oxford and co-head oft he UK based Recovery trial said in an interview with the French online newspaper France-Soir on June 6, „it is 2400 mg in the first 24 hours and 800 mg from day 2 to day 10. It is an 10 day course of treatment in total.“ That makes a total of almost 10 g, with 2.4 g on the first day alone.
In addition, dosing failed to take into account weight, renal and hepatitic function,“ as Meryl Nass points out. „And the 2.4 g in the first 24 hours have given to already very ill, hopitalized COVID-19 patients, a potentially lethal dose.“
Landray being asked, „Are there any maximum dosage for hydroxychloroquine in the UK?,“ Landray answered in all seriousness: „I would have to check but it is much larger than the 2400mg, something like six or 10 times that.“ And then: „Are there any doses considered lethal for hydroxychloroquine in the UK by the Medicines and Healthcare products Regulatory Agency, MHRA?“ Landray: „The treating doctors did not report that they thought any of the deaths were due to hydroxychloroquine. We did not stop the [hydroxychloroquine] arm not because of safety but because it doesn’t work. For a new disease such as Covid, there is no approved dosing protocol. But the HCQ dosage used are not dissimilar to that used, as I said, in for example amoebic dysentery.“
The chief investigator of the Recovery trial, Peter Horby, claimed that France Soir misinterpreted Landray’s comments, but France Soir could completely refute the criticism.
Hence, Landray’s statements create only head shaking, not to say consternation. Not only the UK maximum recommended dosage for hydroxychloroquine with a maximum daily dosage recommendation of 6.5mg per kg of active ingredient, i.e. approximately 500mg per person per day, for known pathologies, had not been respected. And the dosage in the UK Recovery trial for the first 24 hours (2,400 mg) is even higher than the L’autorisation de mise sur le marché (AMM) in France considers the overdose rate at 25mg/kg of hydroxychloroquine, i.e. for a 75kg patient, 1875mg for one day, requiring immediate emergency hospital care.
Furthermore, the Recovery dosage is well above that recommended by the World Medical Association (WMA) in France, as France-Soir reported in its article „Recovery trial: Brexit and overdose“ on June 8, 2020.
The Recovery and Solidarity trials abruptly ended their hydroxychloroquine studies on June 5 and June 17, respectively—coincidentally as people began noticing the excessive doses, especially on Twitter (hashtag #Recoverygate).
The strange thing about it is that still on May 28, the Recovery Control Committee indicated that there was no problem with hydroxychloroquine and therefore recommended that recruitment should be continued without interruption until the next meeting, scheduled for June 11. And this, although on May 22, a Lancet study over 96,000 patient records revealed a much higher death rate in patients receiving hydroxychloroquine and an even higher death rate in subjects receiving hydroxychloroquine plus a macrolidesuch as azithromycin than in the control group.
But the bad news just increased. On May 29, the Indian Council of Medical Research had alerted the WHO about the incredibly high dosing of hydroxychloroquine in the Recovery trial, being four times higher than that used in the indian trials. And on June 4, the UK’s Medicines and Healthcare products Regulatory Agency asked Recovery to look at the data for hydroxychloroquine. The French Minister of Health, by the way, had done the same on May 23, 2020. Four days later the government decided to stop the use of hydroxychloroquine after receiving an adverse report on its use by the National Agency for the Safety of Medicines and Health Products.
Retraction of the Lancet’s hydroxycholoroquine study:
bad aftertaste
Then, on June 4, the Lancet retracted its comprehensive study showing the the high lethality of hydroxychloroquine (plus an antibiotic).
You just ask yourself: What is actually going on here? Something „sucks out loud here.“ The Lancet study has been retracted after independent peer reviewers informed three study-authors that Surgisphere, a Chicago-based company providing and summarizing the raw hospital patient data, would not transfer the full dataset, client contracts, and the full ISO audit report to their servers for analysis. But how realistic is it to assume that the authors of the study—among them cardiologist Mandeep Mehra of Harvard University said to be „one of the stars of the field” and „as straight an arrow as you can find“—compiled it without having studied the raw data and that this study has gone through the peer review process and has been approved for publication without the data having been previously reviewed?
For example, „things like the number of cases that they were claiming out of Australia when the Australian cases weren’t even that high at that time—well, that’s something that a really eminent journal like The Lancet should have been able to pick up on with their peer review process,“ states Roger Lord, a Research Fellow with The Prince Charles Hospital in Brisbane and lecturer in medical sciences at The Australian Catholic University.
This gives rise to the thought: Was it even „necessary“ to withdraw this study? Imagine, what had happened if the Lancet study had not been labled as dubious or even fake, „then of course you’d have a lot of collateral damage in terms of patients not surviving the treatment,“ as Lord points out. Indee, this would have been a kind of a final proof that hydroxychloroquine administered in high doses is a potential „killer“ and thus had finished off the lives of countless patients all over the world. And then, wouldn‘t it also have been much more difficult to get out of the affair with the Recovery Study’s lethal data on hydroxychloroquine?
Or maybe it was a double game: First, on May 22, hydroxychloroquine was demonized by publishing a Lancet study in order to take other drugs such as remdesivir out of the line of fire—and then, on June 5, hydroxychloroquine was taken out of the line of fire by the retraction of the Lancet study as well as by the termination of the Recovery and Solidarity trials (June 5 and 17) by claiming this drug is not effective (instead of telling the truth that this drug has been administered in potentially fatal doses), which in turn caused so much discussion and confusion that the topic “lethal drug effects“ fell out of sight.
Martin Landray, co-head of the UK Recovery study is „incompetent and dangerous“
Another very important question is: How could Landray in all seriousness claim regarding the maximum dosage for hydroxychloroquine in the UK, „I would have to check but it is much larger than the 2400mg, something like six or 10 times“? About this, Christian Perronne, professor of infectious and tropical diseases, pointed out to France Soir:
„In 1975, when I did my medical internship at the Claude Bernard hospital, which was the temple of infectious diseases, I saw a lot of amoebiasis and chloroquine was no longer used to treat that disease. It is the first time that I learn [from Martin Landray] that we use hydroxychloroquine in amoebic dysentery, in super-toxic doses for humans. The classic treatment for colonic amoebiasis is the hydroxyquinoline combination of tiliquinol and tilbroquinol, the trade name of which is Intetrix.“
This is why Perronne thinks „Landray confused hydroxychloroquine with hydroxyquinoline. This man, who calls himself a doctor, is incompetent and dangerous. This is scandalous.“
The comment of France Soir: „British friends, you may be leaving Europe (much to our regret), but your government seems to serve you with a lie.“
The question remains, why did Landray tell France Soir hdyroxychloroquine was not lethal and that they stopped the hydroxychloroquine „arm not because of safety but because it doesn’t work“?
And the answer is that the mortality rate of the comparison group of the hydroxychloroquine arm (randomized to standard of care) in the Recovery trial was 23.6% und was therefore not much lower than in the subjects receiving hydroxychloroquine (25.7%). But there is something very odd here because the 23.6% are unusually high.
„This rate is 18.1% in France and 12.9% in Bouches-du-Rhône (department where Didier Raoult is located),“ as France Soir writes.
In a study published in the Journal of the American Medical Association on May 11, 2020, on severe hospitalized patients comparing hydroxychloroquine plus azithromycin with hydroxychloroquine alone, with azithromycin alone and neither drug, the value was 12.7%. Another study published in the New England Journal of Medicine shows a mortality rate of 32.3% for the hydroxychloroquine group and 14.9% for the control group.
The latter two studies focues on the New York state. That is to say, we have the simple result that twice as many patients died inNew York area when they received hydroxychloroquine.
Who thinks it can’t get any worse, is mistaken. There had been initiated another study, named REMAP, that targets patients who are on a ventilator, or in shock, i.e. near death—using the same hydroxychloroqzuine loading dose (2.4 g in the first 24 hours) as the Recovery and the Solidarity trial and 6.4 g total within six days. But it is even worse for the following reasons, as physician Meryl Nass outlines:
1. As a participant, you have to be close to death, either on a ventilator or in shock, on pressor medications, to be included in the trial, according to the trial documents.
2. You may receive hydroxychloroquine alone, or hydroxychloroquine in combination with 2 more drugs, lopinavir/ritonavir, which, as mentioned, may not only be fatal themselves. Yet lopinavir/ritonavir predisposes to QT prolongation, as does hydroxychloroquine(QT prolongation is a measure of delayed ventricular repolarisation, which means the heart muscle takes longer than normal to recharge between beats). And the drug label states, “Avoid use in combination with QTc- or PR-interval prolonging drugs.”
3. Patients who are in shock or on a ventilator may be unable to give their consent to enroll in a clinical trial. But the trial investigators have deemed that consent may not be required: “For patients who are not competent to consent, either prospective agreement or entry via waiver of consent or some form of deferred consent can be applied, as required by an appropriate ethical review body.”
4. For patients too sick to swallow a pill, the drug will be administered via a feeding tube. This could entail an extra procedure for patients.
The Remap trials took place at 200 sites in 14 countries, among them Belgium, the Netherlands, Spain, the UK, and the USA, all countries with an excess mortality over a relatively short period of time.
The remdesivir scam
Finally, a word about remdesivir, which was approved on May 2, 2020 in the context of COVID-19 for emergency use only. A few days before, the NIAID director Anthony Fauci claimed that a study found remdesivir would reduce recovery time and reduce mortality. But this can only be described as another scandal in which Fauci plays a central role.
An article of the Alliance for Human Research and Protection (AHRP)—“Fauci’s Promotional Hype Catapults Gilead’s remdesivir”—brought up the following painful subject:
“Fauci has a vested interest in remdesivir. He sponsored the clinical trial whose detailed results have not been peer-reviewed. Furthermore, he declared the tenuous results to be ‘highly significant,’ and pronounced remdesivir to be the new ‘standard of care.’ Fauci made the promotional pronouncement while sitting on a couch in the White House, without providing a detailed news release; without a briefing at a medical meeting or in a scientific journal—as is the norm and practice, to allow scientists and researchers to review the data. When he was asked about a recently published Chinese study on remdesivir, in The Lancet (April 29th, 2020); a trial that was stopped because of serious adverse events in 16 (12%) of the patients compared to four (5%) of patients in the placebo group, Dr. Fauci dismissed the study as ‘not adequate.’”
What Fauci also failed to disclose to the public in his promotional pronouncement of remdesivir was that the primary outcomes of the study that led to its emergency use approval were changed on April 16, 2020. Changes in the primary outcome are posted on clinicaltrials.gov. Where previously there was an 8-point scale, which also included the deceased patients, from then on there has been only a 3-point scale, which leaves the deceased patient out of the equation and which at the same time only measures the time until recovery or being released from the hospital.
The first megastar who was labelled as COVID-19 patient and died after the administration of remdesivir was Roy Horn, the magician legend. In fact, he died in Las Vegas on May 8, only six days after the emergency admission of remdesivir, at the age of 75. But the German-born man was in such poor health that it seems just absurd to ignore factors unrelated to a virus as the cause of his sad demise.
In December 2016 Horn was diagnosed with advanced skin cancer, “chemotherapy and radiation therapy were supposed to help, but they additionally weakened him,” as German glossy Bunte reported on its Website. “He had to take strong medication every day. A friend: ‘Before dinner Roy threw in all the pills like Smarties. Not only against the cancer he fought, but also against the pain he had since the tiger attack almost 17 years ago.”
And then Horn took remdesivir. But it is only solidly proven for this medication that it inhibits the cell reproduction in the body as well as that it can cause a multiorgan dysfunction, a septic shock (fatal blood poisoning) or also an acute kidney failure—which all the more can have fatal effects for a seriously ill old person. This justifies the conclusion that the already terminally ill and heavily medicated horn died a tragic and sad premature death not despite but because of the administration of remdesivir.
Let’s listen at the end to what Sir Frank Macfarlane Burnet, the Australian Nobel laureate for medicine, said 50 years ago. It seems more relevant than ever:
„The real challenge of the present day is to find remedies for these diseases of civilization. But nothing that comes out of the labs seems to be significant in this context; laboratory research’s contribution has practically come to an end. For someone who is well on the way to a career as a lab researcher in infectious disease and immunology, these are not comforting words.”
– – – – – – –
Torsten Engelbrecht is an investigative journalist from Hamburg, Germany. In 2020 the updated version of his book „Virus Mania“was published (co-authored by Claus Köhnlein, MD). In 2009 he won the German Alternate Media Award. He was a member of the Financial Times Deutschland staff and has also written for the OffGuardian, The Ecologist, Rubikon, Süddeutsche Zeitung, and many others. See www.torstenengelbrecht.com.
Claus Köhnlein, MD, is a medical specialist of internal diseases. He completed his residency in the Oncology Department at the University of Kiel, Germany. Since 1993, he has worked in his own medical practice, treating patients who are skeptical of antiviral medications. Together with Torsten Engelbrecht he wrote the book „Virus Mania“ (updated in 2020).
Source…